One of the most common types of cancer in the brain is known as metastasis to the brain [1], also referred to as ‘brain metastases,’ secondary brain tumors, or simply ‘brain mets.’ Metastatic brain tumors are cancer that has spread to the brain from other parts of the body, like the breast or the lungs, usually through the bloodstream [2]. Brain metastases are more common in adults than children and occur equally in men and women. 10-20% of patients have only one secondary brain tumor, but the vast majority of patients (80+%) typically have more than one metastatic tumor [3]. Brain metastases are considered malignant forms of cancer.
Since they are different, it is important to distinguish between brain cancer and metastasis to the brain. Brain cancer, also known as primary brain cancer, is a tumor that starts in the brain. Metastatic cancer spreading to the brain, on the other hand, is more common than primary brain cancer [4].
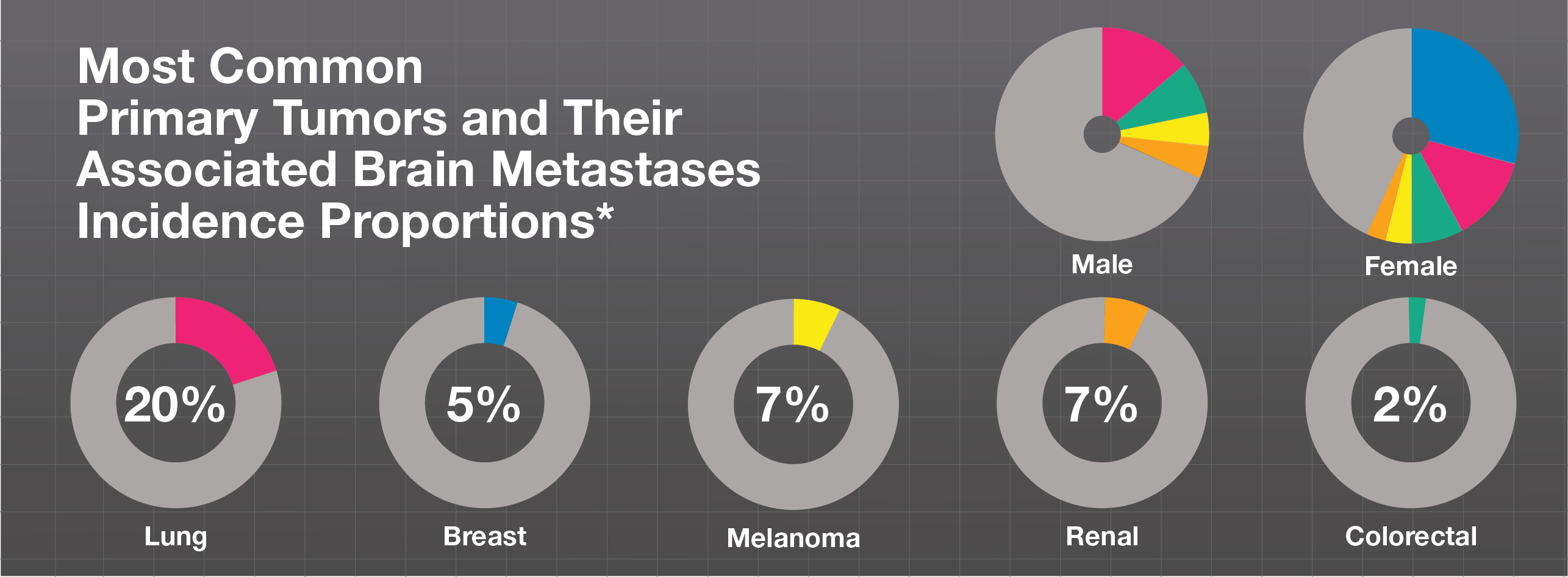
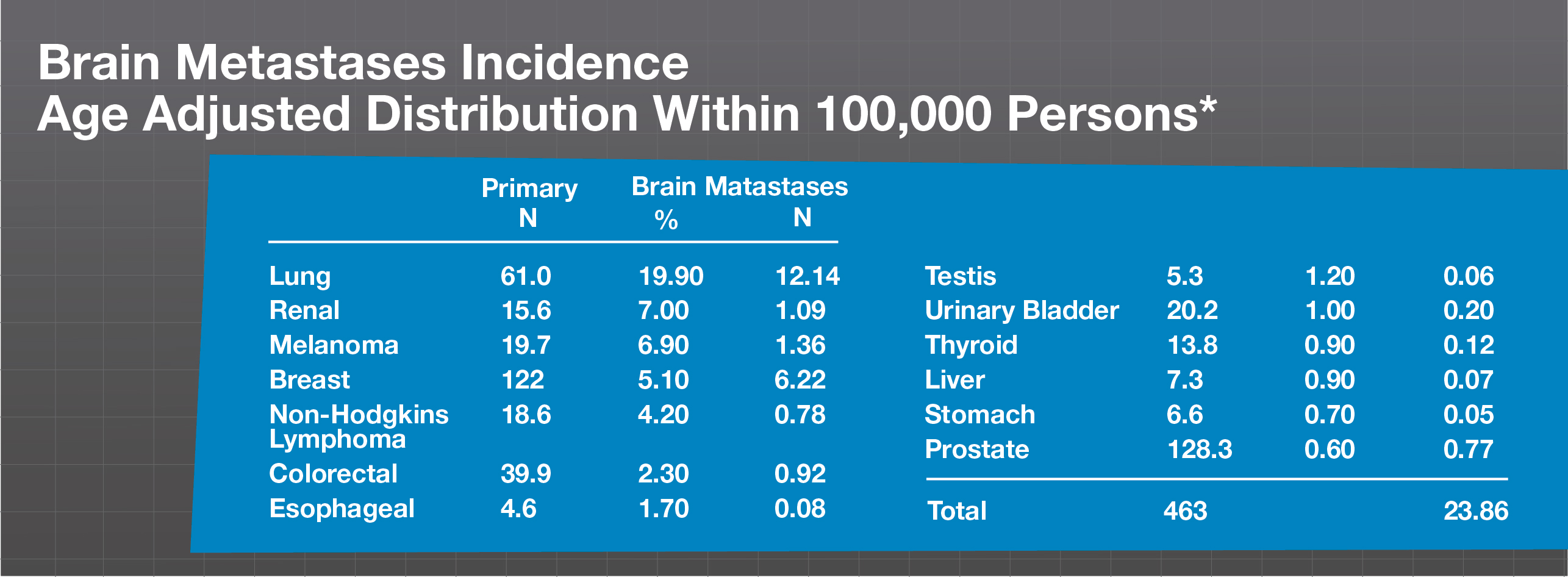
While there are many statistics about which cancers most commonly spread to the brain, we’ve used the U.S. National Program of Cancer Registries and secondary tumor incidence rates [5] to show how often different primary cancers develop into brain metastasis.
It’s estimated that 20-40% of all patients diagnosed with a primary cancer will develop a secondary cancer in the brain, called metastasis.[6] Today, more people are being diagnosed with brain mets because improvements in medical imaging are helping with early diagnosis. In addition, better and more effective treatments are controlling primary cancers and prolonging life, which can allow time for the primary cancer to migrate to the brain. [7]
Advanced technologies and treatment options are helping improve survival rates and quality of life for patients, helping them live longer, fuller lives with better control of their cancer. As a result, death rates are going down, while length of survival is improving in advanced stages of the disease. [8-10]
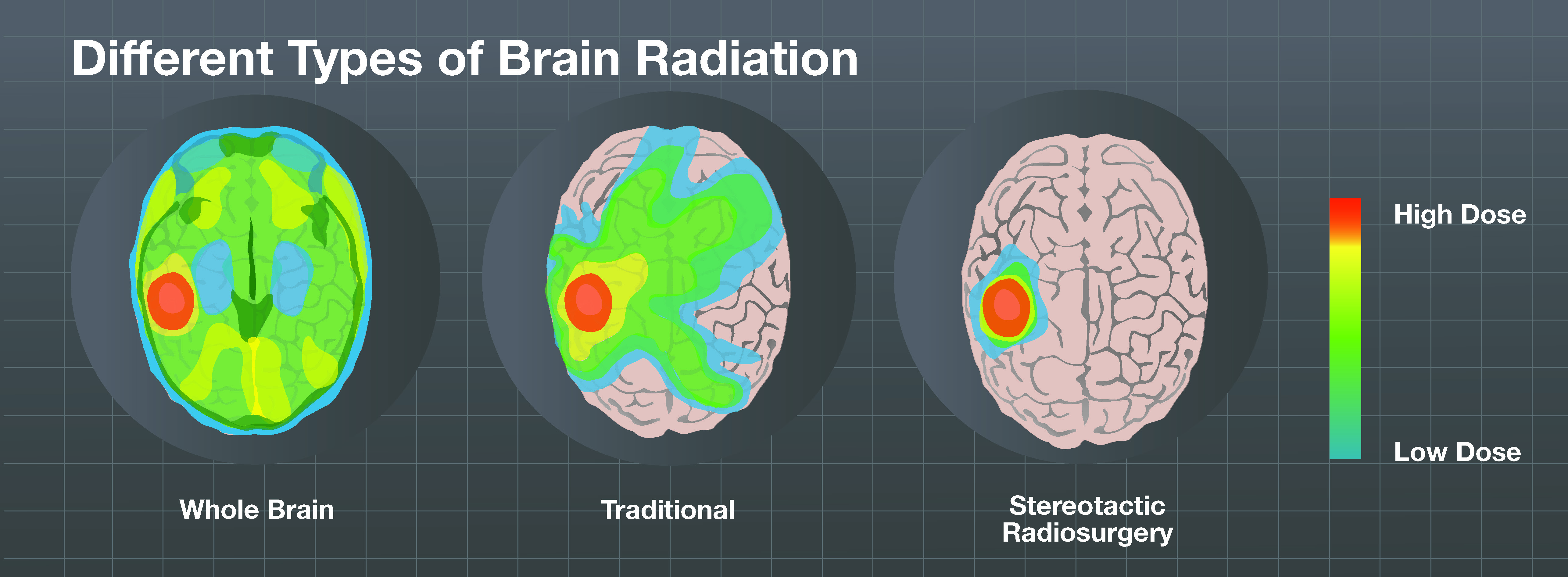
Patients should discuss quality of life and ‘preservation of cognitive function’ when analyzing brain metastasis treatment options such as surgery, whole brain radiation and stereotactic radiosurgery. Over the last decade, studies have been conducted that suggest that some patients can be treated with stereotactic radiosurgery (SRS) alone without whole brain radiation therapy. Memory and learning are important components of any patient’s quality of life, and we now know that SRS alone is a viable and effective treatment consideration. [11, 12]
See How are Brain Metastases Treated for an overview of treatment options.
Everyone’s battle with brain metastases is different and treatment technologies should be part of an overall cancer discussion with your oncology team.
[1] Gavrilovic, I. T. & Posner, J. B. Brain metastases: epidemiology and pathophysiology. J. Neurooncol. 75, 5–14 (2005)
[2] Fidler, I. The pathogenesis of cancer metastasis: the ‘seed and soil’ hypothesis revisited. Nat. Rev. Cancer 3, 1–6 (2003)
[3] American Brain Tumor Association
[4] American Association of Neurological Surgeons
[5] Davis et. al. (need to find this one)
[6] J. Wong, A. Hird, A. Kirou-Mauro, J. Napolskikh, E. Chow. Quality of life in brain metastases radiation trials: a literature review. Current Oncol., 2008 Oct; 15(5): 25–45.
[7] http://www.ncbi.nlm.nih.gov/pubmed/22012633
[8]Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D: Global cancer statistics. CA Cancer J Clin 61: 69-90, 2011
[9]Kohler BA, Ward E, McCarthy BJ, Schymura MJ, Ries LA, Eheman C, Jemal A,Anderson RN, Ajani UA, Edwards BK: Annual report to the nation on the status of cancer, 1975-2007, featuring tumors of the brain and other nervous system. J Natl Cancer Inst 103: 714-736, 2011
[10] Siegel R, Ward E, Brawley O, Jemal A: Cancer statistics, 2011: The impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin 61: 212-236, 2011
[11] Gaspar L, Scott C, Rotman M, Asbell S, Phillips T, Wasserman T, McKenna WG,Byhardt R: Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys 37: 745-751, 1997
[12] Nicholas F. Marko, Robert J. Weil: Neurocognitive considerations in the treatment of brain metastases. Nature. Vol 7 185-186, April 2010